Flow Cytometric and Morphologic Abnormalities in Myelodysplastic Neoplasms (MDS)
Download PDF
Myelodysplastic neoplasms (MDS)—abbreviated in acknowledgment of the historic use of the term myelodysplastic syndrome—are clonal bone marrow disorders characterized by ineffective hematopoiesis (blood production), leading to peripheral blood cytopenia(s) and a variable risk of transformation into acute myeloid leukemia (AML).1 The defining features of MDS include:
- Morphologic Dysplasia: Evidence of abnormal maturation in one or more hematopoietic lineages (erythroid, myeloid or megakaryocytic) visible on microscopic examination.2
- Cytopenias: Low blood counts (e.g., anemia, neutropenia, thrombocytopenia).3
- Genetic Abnormalities: Highly prevalent cytogenetic abnormalities and somatic mutations in myeloid-associated genes.
The Role of Flow Cytometry in MDS Diagnosis
Flow cytometry is a critical tool in the workup of suspected MDS, serving multiple essential functions:
- Exclusion of Other Neoplasms: Effectively ruling out other hematopoietic malignancies that may present with cytopenias.
- Supportive Evidence of Dysplasia: Occasionally, flow cytometry can offer direct supportive evidence of abnormal maturation by revealing aberrant cell marker expression or unusual immunophenotypic patterns, which can prompt further focused microscopic scrutiny.4
- Blast Enumeration: Providing an accurate and objective estimation of the relative percentage of blasts in the bone marrow, which is crucial for risk stratification and diagnosis (e.g., classifying MDS with low vs. increased blasts).
Case Study: Aberrant Antigen Expression as a Diagnostic Clue
We present a case that demonstrates how flow cytometric abnormalities can provide early clues indicating a diagnosis of MDS.
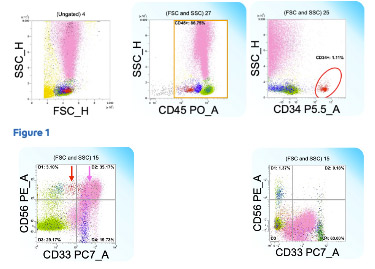
The flow plots seen to the right are derived from the bone marrow aspirate of a patient presenting with unexplained cytopenia.
Color Key: Neoplastic CD34+ myeloblasts are highlighted in red. Granulocytes are pink, lymphocytes are light green, mature monocytes are dark green, and non-neoplastic CD34- myeloblasts are blue.
- Initial Observation: While the relative number of blasts is not overtly increased, they exhibit an abnormal expression of CD56 (see red arrow in Figure 2). An comparative example of normal bone marrow is provided (Figure 2, right image).
- Granulocyte Abnormality: Crucially, the maturing granulocytes also display aberrant CD56 expression (pink arrow). CD56 expression is highly abnormal in the myeloid and blast compartments, serving as an important immunophenotypic clue to an underlying myeloid neoplasm, such as MDS or AML.
Cytogenetic, Molecular and Morphological Correlation
- Cytogenetics: Demonstrated an abnormality, specifically del(20q), a recurrent abnormality commonly associated with myeloid neoplasms.
- Next-generation Sequencing (NGS): Revealed multiple gene mutations frequently seen in myeloid neoplasms.
- Morphologic Analysis: Examination of the aspirate smear and biopsy confirmed significant dysplasia, most notably in the megakaryocytic lineage.
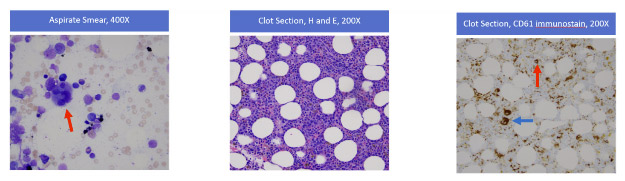
Key Morphologic Findings:
- Megakaryocytic Dysplasia (Aspirate): The bone marrow aspirate smear showed abnormally small megakaryocytes, some with abnormal nuclear lobation (left image, indicated by the red arrow).
- Marrow Cellularity (Core/Clot): Hematoxylin and Eosin (H&E) stains of the clot section (middle image) and core biopsy (not shown) revealed marrow hypercellularity for the patient’s age, which is characteristic of MDS.
- Immunohistochemistry: Because the abnormally small megakaryocytes were difficult to identify on H&E stains, a CD61 stain was performed. This megakaryocyte marker highlighted that while some relatively normal megakaryocytes were present (right image, blue arrow), the majority were abnormally small (micromegakaryocytes) (right image, red arrow); these findings meet criteria for MDS.
Conclusion: The total workup supported a diagnosis of “MDS with low blasts” (WHO Classification, 2022)5
Flow Cytometry as a High-Value Partner
This case powerfully illustrates how the identification of aberrant immunophenotypic patterns (e.g., abnormal CD56 co- expression on blasts and granulocytes) by flow cytometry can help provide clues to the presence of MDS. These clues guide the pathologist, focusing their attention on finding the often subtle diagnostic features of dysplasia on microscopic examinations and pursuing critical confirmatory studies, such as cytogenetics and NGS. Flow cytometry, therefore, is a high-value partner in the definitive diagnosis and classification of myelodysplastic neoplasms.
See pdf for sources.Sigue leyendo Download PDF