Principles of Hemostasis, Part I
Download PDF
The primary principle of hemostasis is to minimize blood loss at sites of vessel injury by forming a thrombus (clot) and at the same time maintaining blood flow. To achieve this, there is a highly regulated, fine-tuned interaction of multiple processes, involving the blood vessel wall (principally the endothelium), platelets and non-cellular blood constituents.
The core elements of hemostasis include blood vessel constriction, platelet activation, coagulation and fibrinolysis. All of these processes are initiated at the same time in response to blood vessel injury. Damage to the endothelial cell lining of the blood vessel results in exposure of collagen which, under normal circumstances, is not in contact with the blood. When circulating platelets come into contact with collagen they are activated and start to stick to the damaged surface. At the same time, a substance called tissue factor is also exposed which activates the coagulation cascade resulting in the formation of a fibrin clot. Platelet adhesion and activation is conventionally known as primary hemostasis and the process of coagulation and fibrin formation is termed secondary hemostasis.
Normal hemostasis depends on the interaction of the following:
- blood vessel
- platelets
- coagulation system
- fibrinolytic system
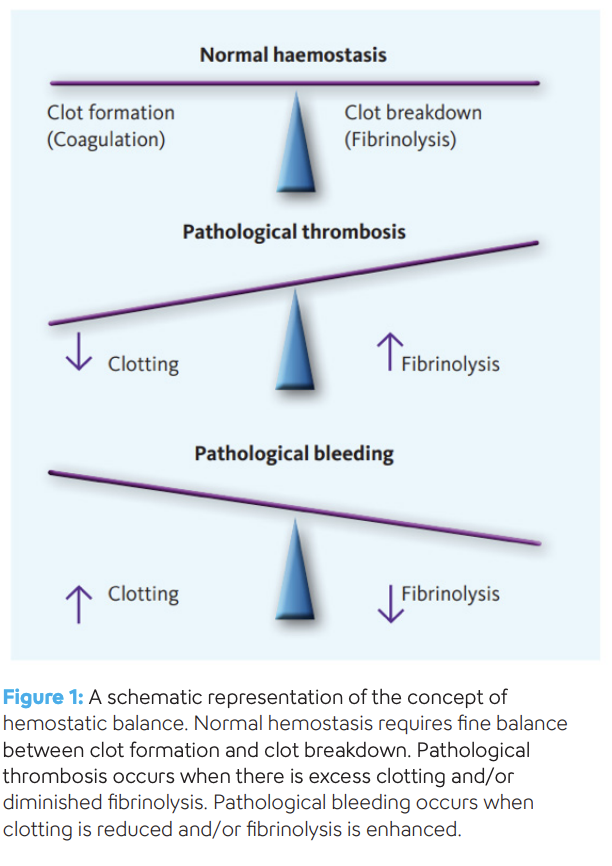
A defect in one or more of these systems will result in either a bleeding disorder or a tendency to clot. Despite the complexities of the control of hemostasis, ultimately the outcome is, quite simply, a matter of balance between clot formation and clot breakdown, both of which in turn are influenced by blood flow (or stasis), the vessel wall and the constituents of the blood (Fig. 1, pdf)).
This article describes the physiology of primary hemostasis. To learn about the coagulation and fibrinolytic systems, read “Principles of Hemostasis, Part II”.
The blood vessel
The blood vessel wall, which is lined with endothelial cells, is the first line of defense for normal hemostasis. The endothelium is a highly regulated ‘organ’ in that it is responsible for ensuring that blood remains fluid at all times so that flow continues without hindrance. The surface is therefore regulated to be highly ‘anticoagulant’ most of the time. However, at the first sign of injury where blood loss could be incurred, the endothelium switches to be highly ‘procoagulant’.
Platelets
Platelets are produced in the bone marrow, then enter peripheral circulation where they have a life span of about 10 days. Platelets have a very complex structure which facilitates the critical role that platelets play in the normal physiology of hemostasis. The major components of the platelet include the surface membrane (composed mainly of phospholipids), intracellular granules, surface receptors and the canalicular system.
Ordinarily, platelets circulate without interacting with the blood vessel wall or any blood constituent proteins. However, at sites of blood vessel damage, platelets stick to a variety of structures via a multitude of platelet surface receptors.
Von Willebrand factor (VWF) is a plasma protein that functions to act as an anchor for platelets at sites of injury. VWF and platelets ordinarily do not interact, but once VWF has bound to subendothelial tissues, it changes its own structure which causes the platelets to bind tightly. The bond takes place via one of the major surface receptors of the platelet, which in turn triggers multiple reactions inside the platelet leading to ‘activation’ of the platelet.
Platelet activation includes several key end points:
Shape change – Platelets undergo a shape change from disc-like to flattened, spread out structures with multiple finger-like extensions. This physically assists in plugging the hole in the vessel wall. Platelets are able to do this because they stores an abundance of ‘excess membrane’ in the form of the canalicular system. This canalicular system is connected to the outside of the platelet and when activated, this excess membrane is pushed to the outside thereby greatly increasing the surface area.
Granule release – Platelets contain granules that are secreted when they are activated. These granules contain a number of key elements, such as factor V, VWF and calcium which further amplify the hemostatic process.
Membrane flip-flop – Platelet activation results in an irreversible flip-flop of its bilayer membrane resulting in the exposure of phospholipids (especially phosphatidylserine) to the plasma which are normally housed primarily within the inner leaflet of the platelet membrane and therefore separated from plasma proteins. This is a critical step in the hemostatic process as phospholipid is an essential element in the support of the coagulation cascade.
Fibrinogen receptor – Another vital consequence of platelet activation is the induction of a shape change in the main surface receptor for fibrinogen. As the fibrinogen molecule has two identical arms, one fibrinogen molecule is able to bind to fibrinogen receptors on adjacent platelets thereby linking them together. The overall effect of this is that there is now a physical seal comprising of stretched out platelets which are tethered to collagen in the vessel wall at the site of injury. The primary platelet plug by itself is however only a temporary seal, and the formation of a proper clot is needed in order to seal the vessel wall securely while the damaged vessel repairs itself. The exposed phosphatidylserine on the surface of activated platelets is ready to support the coagulation cascade.
Sigue leyendo Download PDF

