Automating Body Fluid Analysis for Increased Efficiency
Download PDF
The association between body fluids and human disease was first popularized around 400 BC when Hippocrates taught that illness is the result of an imbalance in the body’s “four humors” or liquids. This theory, termed humoralism, persisted in the medical community for over two thousand years before it was fully discarded for modern discoveries in biology and cellular pathology.1 Our present understanding of the role of various body fluids has come a long way from the teachings of the ancient Greeks. Modern medicine recognizes many more than four body fluids, but relatively few are routinely analyzed as part of the diagnostic process.
Body fluid can be loosely defined as a biological liquid that originates from inside the human body. This represents a large category that includes everything from blood and urine to sweat and tears. Because blood and urine testing is commonplace in the clinical laboratory, many analyzers have been developed to rapidly and accurately process such specimens; however, until fairly recently, analysis of other fluid types relied on time-consuming, manual procedures. The Sysmex XN-Series™ analyzers have a dedicated body fluid mode that is capable of rapid and accurate analysis of select body fluids utilizing direct current technology, flow cytometry, and proprietary algorithms.
Types of body fluid & clinical significance
Although body fluids serve many diverse and necessary functions in the body, aside from blood and urine, few are commonly collected for diagnostic purposes. The three that this paper focuses on— serous fluid, synovial fluid, and cerebrospinal fluid— all function to protect and lubricate the structures they surround as well as provide nutrients and remove waste products. However, the implications of abnormal findings in each of these fluids are varied.
Serous fluid
Serous fluids are those that are found inside the body’s cavities. The term serous comes from the fact that these fluids are normally clear and pale yellow, much like blood serum. The function of this body fluid is to lubricate the organs to reduce friction from movement. Serous fluids commonly analyzed in the clinical laboratory include: pleural fluid from the lung cavity; peritoneal fluid (also called ascites) which is fluid that has accumulated in the abdominal cavity; and pericardial fluid from around the heart. Normally, very little fluid is present in these cavities, but pathologic conditions can cause increased buildup of fluid at these sites.
The cause of serous fluid accumulation, or effusion, can be narrowed down by determining if the fluid is a transudate or an exudate. Transudates are produced by increased pressure in the blood vessels; as the hydrostatic pressure rises, fluid is squeezed out of the vessels and collects in the surrounding cavity. Conditions that may cause this to happen are congestive heart failure, liver cirrhosis, and kidney failure, among others.2 Exudative effusions, on the other hand, accompany inflammatory processes. During inflammation, spaces form between the cells of the tissue walls to enable passage of inflammatory cytokines which also allows fluid to escape into the spaces surrounding the organs. Exudates are commonly caused by malignancy, embolism, or infection.2 Laboratory testing to determine the origin of the accumulated fluid includes comparison of the serous fluid protein and lactate dehydrogenase (LDH) levels to those in the patient’s serum as well as white blood cell counts which will typically be elevated in exudative fluids.
If the fluid is determined to be exudative in nature, it is very important to discover the specific cause of the effusion. Additional laboratory evaluation, including fluid cell count with differential, cytology testing, and culture with Gram stain is helpful to identify white blood cells (WBCs) that often accompany infection or inflammation, malignant cells, or bacterial or fungal pathogens.
Rarely, a peritoneal or pleural lavage may be collected to look for diagnostic information in the absence of a significant effusion. It was once common practice to evaluate patients with blunt abdominal trauma by performing a peritoneal lavage for the presence of RBCs, though this procedure has widely been replaced by the use of computed tomography (CT) and ultrasound imaging.3 Pleural lavage cytology studies many times detect malignancies of the pleural cavity more reliably than pleural fluid analysis, presumably because of cell degeneration in the exudate.4
Dialysate fluid analysis can also be useful to diagnose infection in patients undergoing continuous ambulatory peritoneal dialysis (CAPD) or automated peritoneal dialysis (APD). These procedures are alternatives to hemodialysis for some patients, and the post-filtration product, which contains peritoneal fluid, can be analyzed for the presence of white blood cells or organisms which would indicate infection of the peritoneum.
Synovial fluid
Synovial fluid is also commonly tested by many clinical laboratories to diagnose various joint diseases. Synovial fluid is an ultrafiltrate of blood plasma that combines with high molecular weight hyaluronic acid to form a viscous fluid that cushions and lubricates the cartilaginous bone surfaces in movable joints. Diseases of the joints are sometimes classified according to their underlying causes: non- inflammatory (degenerative); inflammatory (including crystal-induced inflammation); infectious; and hemorrhagic.5
Analysis of synovial fluid will typically include a cell count with WBC differential, culture and Gram stain, and polarized light microscopy for crystal identification. The cell count may or may not include a red blood cell (RBC) count, depending on the suspected diagnosis or policy of the performing laboratory. Crystal examination by polarized light microscopy allows for detection of monosodium urate crystals which are diagnostic of gout, or calcium pyrophosphate dihydrate crystals which may be seen in pseudo gout. Some authors suggest pre-treating synovial fluid with hyaluronidase to decrease the viscosity, allowing for more uniform distribution of cells when counting and preparing slides for the WBC differential.6,7 It is important to note, however, that hyaluronidase may interfere with crystal examination, and therefore should only be used for the cell count portion of analysis.
An internet search of several clinical laboratory testing menus shows that reference ranges for synovial fluid cell counts vary. White cell results up to 200 cells/µl are considered within normal ranges for many labs, however, some laboratories choose not to publish ranges or state that reference ranges are not established for synovial fluid samples. This may be due to lack of “normal” fluid samples for reference range evaluation or scarcity of published reference range studies. Red blood cells should not be present in normal synovial fluid, but oftentimes are seen during analysis as contamination from the fluid collection process. A traumatic collection may complicate diagnosis of a hemorrhagic condition.
In addition to the white blood cell count and differential, inflammation of the joint may be detected by performing the mucin clot test. Normal synovial fluid will form a stable clot when added to acetic acid due to the hyaluronic acid-protein complex; the presence of inflammatory enzymes in the sample will decrease the integrity of this complex, resulting in weak or absent clotting.8 The mucin clot test, however, is not widely considered as a reliable and useful test for diagnosing inflammatory joint diseases2 and many laboratories have discontinued performing this test.
Cerebrospinal fluid
Cerebrospinal fluid (CSF) is a clear, colorless fluid that fills the subarachnoid space surrounding the brain and spinal column. It primarily acts as a cushion and lubricant for the central nervous system, but also distributes nutrients and removes waste products from the brain.
Indications for testing CSF traditionally include suspected meningitis, subarachnoid hemorrhage (SAH), central nervous system (CNS) malignancy, or demyelinating disease; however, advancements in other diagnostic technologies have made CSF collection less popular for certain diagnostic testing. In the case of SAH, computed tomography (CT) is the primary method of diagnosis with 98 percent sensitivity when performed within the first 12 hours.9
The normal WBC count in CSF is generally agreed upon as < 5/µL in adults and < 30/µL in newborns. RBCs should not be present in CSF, but may be seen during analysis due to contamination from the lumbar puncture procedure. When analyzing spinal fluid for possible subarachnoid hemorrhage, RBC counts should be performed on the first and third tubes collected to observe for lessening of the amount of red cells present, which would indicate a traumatic collection. Recent research has concluded that the absence of xanthrochromia (signifying the breakdown of RBCs in the CSF) and a RBC count of < 2,000 cells/µL excludes the diagnosis of subarachnoid hemorrhage with a sensitivity of 100 percent.10
A sampling of WBC reference ranges for the various types of body fluids are shown in Table 1 (pdf).
Other fluids
In addition to the fluids already mentioned, there are others that may be of clinical importance. Broncho-alveolar lavage (BAL), also referred to as broncho-alveolar washing, may be helpful in diagnosing hemorrhage, malignancies, or infections of the lung.14 Amniotic fluid may be obtained by amniocentesis to evaluate several genetic or developmental problems in the fetus. Hematology departments rarely analyze amniotic fluid except for performing lamellar body counts to assess fetal lung maturity. Neither of these fluid types are cleared for analysis on the XN-Series analyzers.
Analysis of body fluids
As discussed in the previous section, there is a wide array of testing that can be performed on the various body fluids to add information to the diagnostic picture. Each department in the clinical laboratory responsible for performing this testing should be aware of the special considerations when handling body fluid and must develop the standard operating procedures and training plan accordingly. The remainder of this article will discuss the specific processes and concerns that are encountered when performing hematology evaluation of body fluids.

Manual cell counting
Cell counts are often part of the standard testing that is ordered when a body fluid is collected from a patient. Enumeration of the cells present in a fluid sample can help identify possible underlying pathologies that might not be apparent from the patient’s overall clinical picture. The additional information obtained from the white cell differential may lead to - or exclude - a final diagnosis.
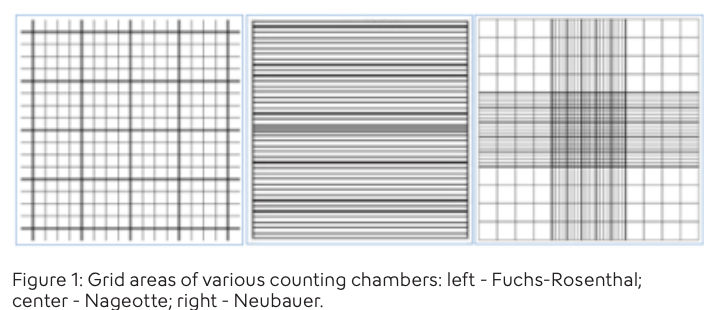
Historically, cell counts were performed using optical microscopy and counting chambers, called hemocytometers, which are designed specifically for accurate quantitation of white and red blood cells. There are numerous chambers available for cell counting – three popular models being Fuchs-Rosenthal, Nageotte, and Neubauer – most of which differ in the design of the calibrated counting area that is etched on the face of the chamber. (Figure 1, pdf) The chambers allow for a precise amount of fluid to be filled and therefore provide a defined volume for cell enumeration.
While manual counting is considered the gold standard, it iscommonly recognized that this procedure has many drawbacks including, but not limited to, high imprecision, long turnaround times, high cost, and need for specially trained personnel.15,6 A potential source of error when counting WBCs and RBCs concurrently is misclassification of cells using bright field microscopy. For this reason, the College of American Pathologists (CAP) includes verification of manual RBC counts with an alternative method as part of their accreditation program requirements.16 Also, distinguishing WBCs from tissue cells is problematic on the hemocytometer, forcing many laboratories to report a “total nucleated cell count” in lieu of a white blood cell count on body fluids.
Automated cell counting

When deciding whether to automate body fluid cell counts, laboratories need to evaluate the advantages and disadvantages of each method. Automation offers many benefits including improved accuracy, precision, faster turnaround times, and standardization of results17 and also eliminates the challenges of extensive training and competency testing of the lab staff. Disadvantages mostly revolve around the technical confines of the analyzer used. Many cell counters used in the clinical laboratory have been evaluated for cell counting of body fluid samples, and some even have body fluid analysis modes incorporated into their equipment. It is important for users to understand the limitations of the technology being used, as well as the manufacturers’ intended use and reportable ranges, before embarking on the automation process. Additionally, when choosing to automate body fluid cell counts, laboratories should provide an alternative procedure for obtaining accurate results when cell counts are outside of the determined reportable ranges.
The first aspect to be considered is the types of body fluid that can be analyzed using automation. If an instrument is validated by the manufacturer for body fluid analysis, the acceptable fluid types should be clearly stated in the analyzer’s instructions for use. The XN-Series Body Fluid mode is cleared for analysis of synovial fluid, pleural fluid, and peritoneal fluid, and the XN-10 analyzer is also cleared for CSF samples in the Body Fluid mode.
It must be noted that whenever a specimen type is being analyzed that has not been cleared for testing on an analyzer, the laboratory must perform studies to prove acceptability for that specimen type.12 The extent of this testing must comply with the regulatory agencies that oversee accreditation of the laboratory performing the testing. This may include comparison of the automated and manual methods, establishment of reference ranges, evaluation of sample stability, and periodic verification of the accuracy and precision for testing of that sample type. Some accreditation agencies also require that laboratories report a disclaimer with results reported on samples that are tested using laboratory developed methods.
A listing of fluid types cleared for analysis on the XN- Series analyzers is shown in Table 2 (pdf).
Another limitation of automated methods may be the chosen analyzer’s reportable range for body fluid cell counts. To understand how to interpret the manufacturer’s stated ranges, we need to understand the analyzer’s limit of blank, limit of detection, and limit of quantitation. The limit of blank (LoB) is the highest count that should be obtained by a cell counter when a blank, or negative, sample is analyzed. The LoB could be verified by analyzing body fluid samples devoid of cells or, in the absence of such samples, diluting reagent.12 The limit of detection (LoD) is the lowest number of cells that can be reliably detected during analysis and is distinguishable from “analytical noise”.18 The LoD should be a value greater than the LoB in order to ensure any events counted truly represent cells in the sample. The limit of quantitation (LoQ) is the amount of cells that can be reliably detected by the analyzer while also meeting any rules for bias and imprecision.19 The LoQ and LoD may be the same, or the LoQ may be higher if the method comparisons show a bias. The LoQ would be considered the low end of the reportable range.
The background limits and reportable ranges for the XN Body Fluid mode are stated in the XN-Series Instructions for Use manual. Background checks are automatically performed and recorded when the body fluid mode is accessed and the data is compared against the stated acceptable limits. If the body fluid white blood cell count (WBC-BF) or red blood cell count (RBC-BF) background count exceeds the acceptable limits, the XN analyzer will automatically launch into a rinse and initiate another background check. The background check will be performed up to three times or until the background results are acceptable. It may be noted that the upper limit for the RBC-BF background check on the XN is higher than the lowest reportable value (LoQ) for that parameter; the result would be valid as long as the preceding RBC-BF background value (or “blank”) is lower than the value obtained on the sample. The laboratory may also want to consider the sample volume required by the analyzer before deciding to automate fluid cell counts. Often minimal sample volume is collected and multiple tests are ordered, so there is limited sample available for analysis. While plating a hemocytometer may require less than 20 µL of fluid, automated cell counters may require up to 1 mL of fluid for analysis. In cases where sufficient sample volume is received, however, the precision and accuracy offered by the automated method may outweigh the benefit of using less volume with the manual method.
Body fluid cell differential

Many procedures for body fluid cell counts include a differential, or ‘diff’, of the cells present. It is up to the laboratory policy to dictate whether only white blood cells or all nucleated blood cells will be included in the cell count and differential. Nucleated cells that may be excluded from the cell count or diff include non-hematopoietic cells such as tissue lining cells (mesothelial cells or synovial lining cells), tumor cells, or macrophages.
The Body Fluid mode on the XN-Series analyzers reports both a body fluid white blood cell count (WBC-BF) and a total nucleated body fluid cell count (TC-BF) as well as a reportable 2-part automated diff that differentiates mononuclear and polymorphonuclear cells using flow cytometry technology.
The purpose of the body fluid differential is to evaluate the types of cells present as well as to determine if any abnormal morphological changes are seen. Frequently, the paucity of cells in body fluid will require concentration of the cells before a diff can be performed. Many procedures for preparing body fluid slides for review involve cytocentrifugation techniques where cells are concentrated in a “button” on a slide using specialized funnels and low centrifugal speed.
After staining, a 100-cell diff may be performed, or in the case of very low cell counts, a predominant cell type may be reported.
Even in samples with low cell counts, a predominant cell type is important to note when the count is of clinical significance. The XN Body Fluid mode is FDA-cleared to report a 2-part differential that discerns mononuclear (MN) cells from polymorphonuclear (PMN) cells; a differential reported this way may support a primary clinical decision in an urgent situation or when an experienced laboratorian is not available.20 In fluids that accumulate as a result of inflammation or an infectious process, the cells will typically be neutrophilic versus mononuclear cells which are seen more regularly in chronic conditions. However, interpreting the significance of the cells present in the differential must be done with caution as neutrophils degenerate more readily in aging body fluid than non-granulocytic cells. It is also important to interpret the cell differential considering possible contamination from peripheral blood during the collection procedure.
In addition to mononuclear cells and PMNs, the XN analyzer also recognizes cells identified as high fluorescing body fluid cells (HF-BF). This population represents large cells that are not uncommon in body fluid samples such as mesothelial cells, synovial cells, and malignant/ tumor cells, or, rarely, large cell clusters. Events in the HF-BF area of the scattergram are included in the TC-BF but not the WBC-BF, as these cells are generally non-hematopoietic. User-defined flagging on the XN makes it possible to generate the “WBC Abn Scattergram” message when any amount of HF-BF cells are detected. When this message is utilized, it may assist laboratories in detecting abnormal or clumped cells.
Digital imaging technology that is used in hematology departments to automate peripheral blood differentials may also be used for simplifying body fluid differentials. Sysmex DI-60™ offers a cell morphology program that is specific to body fluid samples (Figure 2, pdf); this software can classify five different nucleated cell types that are typically found in body fluid, allows users to add reference cells to a digital library, enables tagging and sharing of cell images electronically, and offers a program to ensure staff competency. The use of digital cell imaging software in the laboratory has been shown to increase efficiency in workflow and training activities.21
Challenges of body fluid testing

Similar to other testing performed in the clinical laboratory, the quality of body fluid test results is dependent upon many variables. Training of the laboratory staff in specimen handling procedures and analysis of the sample are key to producing quality diagnostic results. In many cases, automating high complexity testing can yield results superior in accuracy and precision in comparison to manual procedures.7 Additionally, the delicate nature of cells suspended in body fluid requires prompt attention and careful handling to assure full recovery of cells and accurate counts.2
Having a quality sample to analyze is also of utmost importance, however, the responsibility of proper sample collection generally lies outside of the control of the laboratory. Incorrect choice of anticoagulants for the testing requested as well as poor collection technique may complicate interpretation of test results.
Clotted or suboptimal body fluid samples present a challenge for laboratories that are reluctant to reject irreplaceable specimens, and therefore many labs have policies to address the irregularities that may affect body fluid testing results.22
When performing any clinical testing, the possibility of interfering substances needs to be assessed, and this is especially valid for automated cell counting. The XN analyzer utilizes impedance counting principles for RBC-BF enumeration and flow cytometry for performing the WBC-BF counts and the 2-part differential. Particles present in the body fluid such as crystals, yeast, lipids, and debris that may be introduced during joint revision procedures have been known to interfere with automated cell counts.23,24,25 Using algorithms in the WDF scattergram, the XN body fluid mode has the ability to flag when abnormal patterns are recorded from the flow cell; presence of the “WBC Abn Scattergram” message indicates that the automated TNC-BF and WBC-BF counts may be unreliable and the results should be verified with dilution or by alternate methods.
Automated Counting Technology & Case Studies

XN-BF technology
The XN body fluid mode utilizes impedance counting
principles to obtain the RBC-BF results. Particles
passing through the RBC aperture within the range
of 25 – 250 fL may be counted as red blood cells.
The RBC distribution histogram for the XN body fluid
mode is shown in Figure 3 (pdf).
For determination of the WBC-BF and 2-part automated differential, the XN uses Lysercell WDF™ as a RBC lysing reagent and Fluorocell WDF™ to stain RNA and DNA in the nucleated cells. The specimen is then analyzed in the flow cell and the cell events are plotted on the WDF scattergram using the body fluid algorithm. (Figure 4, pdf)
The WDF scattergram plots the cells according to their side scattered light intensity (x-axis) and side fluorescent light intensity (y-axis), which reflect the complexity of the cell and the nucleic acid content, respectively. The WDF channel differentiates mononuclear cells (MN) from polymorphonuclear cells (PMN); the sum of these two populations is reported as the WBC-BF. A third population of cells, the HF-BF or high-fluorescing body fluid cells, plots higher in the scattergram than the MN and PMN populations due to the fact that HF-BF cells contain more nucleic acid than the white cells. All three populations comprise the total nucleated cell count, or TC-BF. It is important to note that although the HF- BF population is included in the TC-BF, it is not itself a reportable parameter.
The XN Data Browser software also displays an extended body fluid differential scattergram, WDF(EXT), which raises the threshold of the y-axis. This allows viewing of the entire HF-BF population which may drift beyond the limits of the standard body fluid WDF scattergram due to excess fluorescence in non-hematopoietic cells. (Figure 5, pdf)
Case study


One milliliter of synovial fluid from an elbow joint
was received in a syringe with a test order for cell
count, differential and crystal examination. A portion
of the fluid intended for cell count testing was
pretreated with hyaluronidase. After an incubation
period in accordance with the laboratory’s operating
procedure, the sample was analyzed in the body fluid
mode on the XN and the results obtained are shown
in Figure 6 (pdf).
The WDF scattergram showed an abnormal distribution pattern and therefore the “WBC Abn Scattergram” message was triggered by the XN. The untreated portion of fluid reserved for crystal examination revealed a marked amount of intra- and extracellular uric acid crystals, indicating the high likelihood of gouty inflammation of the joint.
Because of the abnormal scattergram, confirmation of the WBC-BF count was required and a manual count was performed per lab policy. The manual hemocytometer count showed a nucleated cell count significantly lower than the automated count. The discrepancy between the manual nucleated cell count and the automated TC-BF is due to the marked amount of clusters of uric acid crystals in the sample.
As the highly-refractile crystals pass through the flow cell on the XN the light is scattered and recorded in the scattergram. The events in the scattergram are classified as nucleated cells, however, the non-specific light scatter pattern is interpreted as abnormal by the WDF-BF algorithm, causing the “WBC Abn Scattergram” message to be generated. During manual counting the crystals are not identified as nucleated cells and, therefore, the manual count yields a more accurate cell count.
Summary
Body fluid analysis can provide a significant amount
of information and insight into a patient’s diagnostic
picture. In most cases, automation of body fluid cell
counts offers increased efficiency, accuracy, and
precision when compared to manual methods that
require time and expertise to perform. Knowing
the limitations of the analyzer used is important
when interpreting automated cell count results and
associated histograms and scattergrams. Dedicated
body fluid analysis modes, such as that which is
available on some XN-Series analyzers, deliver the
additional benefit of automatic background checks,
enhanced sample flagging, and specific algorithms
capable of delivering a reportable 2-part differential.
Bibliography
1. Webster’s New World Medical Dictionary, 3rd Ed.
2. Kjeldsberg C, Knight J. Body Fluids. 3rd Ed. Chicago, IL: ASCP Press; 1993.
3. Simon RJ. Diagnostic Peritoneal Lavage. UpToDate website. https://www.uptodate. com/contents/diagnostic- peritoneal-lavage. May 3, 2017. Accessed August 8, 2018
4. Mohamed KH, Mobasher AA, Yousel AI, et al. Pleural lavage: a novel diagnostic approach for diagnosing exudative pleural effusion. Lung. 2000 November-December; 178(6):371-9.
5. Sysmex Europe GmbH. Sysmex Educational Enhancement and Development (SEED) Body Fluids. Sysmex Europe GmbH website. https://www.sysmex. co.za/academy/library/sysmex- educational-enhancement- development.html. Accessed July 10, 2018.
6. Kjeldsberg's Body Fluid Analysis, Page 141, American Society for Clinical Pathology Press, 2015.
7. Seghezzi M, Buoro S, Manenti B, et al. Optimization of Cellular analysis of Synovial Fluids by optical microscopy and automated count using the Sysmex XN Body Fluid Mode. Clin Chim Acta. 2016 November 1;462:41-48
8. McBride LJ. Textbook of Urine and Body Fluids: A Clinical Approach. Philadelphia, PA: Lippincott; 1998.
9. Gorchynski J, Oman J, Newton T. Interpretation of Traumatic Lumbar Punctures in the Setting of Possible Subarachnoid Hemorrhage: Who Can Be Safely Discharged? Cal J Emerg Med. 2007;8:3-7
10. Perry J, Alyahya B, Sivilotti M, et al. Differentiation between traumatic tap and aneurysmal subarachnoid hemorrhage: prospective cohort study. BMJ. 2015;350:H568
11. Kurec A. “Tips from the Clinical Experts.” MLO. 2016 March 23:44-5.
12. Exeter Clinical Laboratory International. https://www. exeterlaboratory.com/test/ transudate-or-exudate/. Accessed December 3, 2018.
13. ClinLab Navigator website. http://www.clinlabnavigator. com/synovial-fluid-analysis. html. Accessed December 3, 2018.
14. American Thoracic Society. Bronchoalveolar Lavage. American Thoracic Society website. https://www.thoracic. org/professionals/clinical- resources/critical-care/ clinical-education/critical-care- procedures/bronchoalveolar- lavage.php. Accessed December 3, 2018.
15. Buoro S, Mecca T, Azzarà G, et al. Cell Population Data and reflex testing rules of cell analysis in pleural and ascetic fluids using body fluid mode on Sysmex XN-9000. Clin Chim Acta. 2016 January 15; 452:92-8
16. College of American Pathologists. Hematology and Coagulation Checklist. CAP Accreditation Program. 2017 August 21.
17. Bourner G, De la Salle B, George T, et al. ICSH guidelines for the verification and performance of automated cell counters for body fluids. Int J Lab Hematol. 2014 Dec;36(6):598-612.
18. Armbruster D, Pry T. Limit of Blank, Limit of Detection and Limit of Quantitation. Clin Biochem Rev. 2008 Aug;29(Suppl 1):S49-S52.
19. CLSI Document EP17-A Protocol for Determination of Limits of Detection and Limits of Quantitation; Approved Guideline. 2008.
20. de Jonge R, Brouwer R, de Graaf M, et al. Evaluation of the new body fluid mode on the Sysmex XE-5000 for counting leukocytes and erythrocytes in cerebrospinal fluid and other body fluids. Clin Chem Lab Med. 2010;48:665-75.
21. Lee L, Mansoor A, Wood B, et al. Performance of CellaVision DM96 in leukocyte classification. J Pathol Inform. 2013;4:14.
22. Cruz F. “Tips from the Clinical Experts.” MLO. 2007 October:42.
23. Fleming C, Bruin M, Russcher H, et al. Liposomal interference on Sysmex XN-series body fluid mode. Clin Chem Lab Med. 2016 Jan;54(1):E19-23.
24. Favresse J, van Dievoet M, De Wolf H, et al. Characterization of Candida spp. Interference on the Sysmex XN-1000 body fluid mode. Int J Lab Hematol. 2018 Apr;40(2):E28-E32.
25. Shu P, Blair J. Cholesterol crystals causing falsely elevated automated cell count. Am J Clin Pathol. 2006 Mar; 125(3):358- 63.
Disclaimer
Some uses or clinical applications described in this paper may not have been cleared by the FDA. It is the clinician’s responsibility to validate any off-label applications for use in routine clinical practice.
Keep reading: Download PDF