Hemostasis - Activated Partial Thromboplastin Time
Download PDF
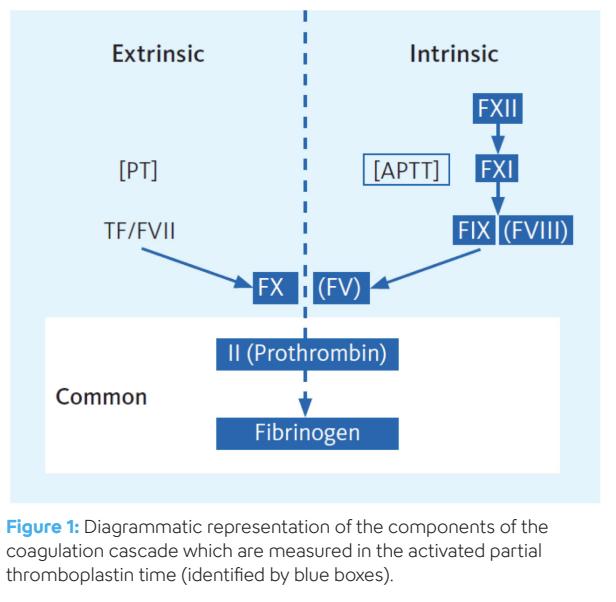
The activated partial thromboplastin time (APTT) is the second most frequently requested coagulation test. The APTT is a laboratory test that is most commonly used to monitor the anticoagulant effects of unfractionated heparin. It is also used to screen for various bleeding disorders caused by deficiencies in the intrinsic coagulation pathway i.e. factor XI, factor IX, factor VIII, factor V, factor II (prothrombin) and fibrinogen.
The word ‘partial’ refers to the fact that the reagent used in the APTT lacks the tissue factor that is a core component in the thromboplastin reagent used in the prothrombin time. It contains only the phospholipid component. The original assay, designed in 1953 to identify classical hemophilia (FVIII deficiency), was called the partial thromboplastin time (PTT) and relied on the glass of the test tube to initiate activation of the intrinsic pathway (referred to as ‘contact activation’). In 1961, this assay was modified to speed up the activation process by adding kaolin which replaced the test tube glass as the activation surface. This is why the clotting test in use today to assess the intrinsic pathway is referred to as the ‘activated’ partial thromboplastin time, namely APTT. The terms PTT and APTT are commonly used interchangeably, although, strictly speaking, APTT should be used.
APTT reagents
APTT reagents have two principal components: an activator and a source of phospholipid. The activator can be either particulate in nature (kaolin, celite or silica) or soluble (ellagic acid). The role of the activator is to provide a negatively charged surface which is required for the activation of the so-called contact factors. The contact factors include high molecular weight kininogen (HMWK), prekallikrein and factor XII (FXII). Kallikrein is formed from prekallikrein through the action of HMWK. During this contact activation phase, FXII is activated to FXIIa with the help of HMWK and kallikrein, and in turn converts FXI to FXIa. Kallikrein is formed from prekallikrein through the action of HMWK. The phospholipids are required to provide a surface for the assembly of the tenase complex (FIXa-FVIIIa), which converts FX to FXa, and the prothrombinase complex (FXa-FVa) which converts prothrombin to thrombin. The phospholipid composition varies in both concentration and source depending on the reagent. The phospholipid may be of animal or plant origin or synthetically manufactured to produce a pure form.
Consequently, this diversity in concentration and composition of APTT reagents results in great variation in their responsiveness to heparin, clotting factor deficiencies and lupus anticoagulants. The variability is further impacted by the type of detection systems used by automated systems (i.e. mechanical versus optical). In view of the lack of uniformity of the composition and reactivity of APTT reagents, it is absolutely essential that each laboratory has a quality control mechanism in place and establishes its own reference range for the interpretation of APTT results generated locally. The choice of reagent must take into consideration the primary indication for APTT testing as some reagents are designed to specifically be sensitive or insensitive to lupus anticoagulants.
Keep reading: Download PDF


