The Role of the Immature Platelet Fraction (IPF) in the Differential Diagnosis of Thrombocytopenia
Download the White Paper
The Value-Driven Laboratory
Immature Platelet Fraction (IPF): An insight into assessment and treatment of platelet disorders
We define the value-driven laboratory as one that meets market demands by providing more and new types of diagnostic information to support the delivery of high quality and cost-effective patient care. This paper sets forth the value of the advanced platelet parameters, the Immature Platelet Fraction (IPF%) and the Immature Platelet Fraction Count (IPF#), to help physicians understand the pathophysiological mechanisms leading to low platelet count. The IPF may help physicians determine in a timelier fashion if a thrombocytopenia is due to decreased platelet production by the bone marrow or increased peripheral consumption/destruction of platelets.
Introduction
The Immature Platelet Fraction (IPF) is a measure of thrombopoietic activity that was first described in 1992 by Ault et al.1, who coined the term “reticulated platelets” to describe large platelets with elevated ribonucleic acid (RNA) content. Reticulated platelets can be an analog to the reticulocytes in red cell populations. Ault’s study, and others have shown IPF to be a stable and reproducible parameter2 and superior to the measurement of reticulated platelets using traditional flow cytometry3,4 for providing information to the physician on the rate of thrombopoiesis. The immature platelet population rises as production and release of platelets increases in the bone marrow. Using a peripheral blood sample, the IPF provides an assessment of bone marrow platelet production similar to how a reticulocyte count provides a measure of red cell production. The IPF result is useful in monitoring patients with thrombocytopenia and helps physicians differentiate thrombocytopenia caused by platelet destruction versus compromised platelet production. Therefore, when using this parameter, physicians may reach decisions on appropriate care pathways in a timelier manner.
An Overview of Platelet Parameters
Platelet Count (PLT)
A normal platelet count (150,000 – 450,000/μL) is vital for the maintenance of hemostasis. Platelet counts of less than 150,000/μL are defined as thrombocytopenic, and spontaneous bleeding not associated with injury has been linked to platelet counts of less than 20,000/μL. Current hematology instruments enable accurate measurement of low platelet counts; however, such a measurement only reflects the circulating platelet count at a specific point in time.
Mean Platelet Volume (MPV)
Historically, some clinicians have used an elevated MPV result to assist in the evaluation of thrombocytopenia, or as a surrogate marker for platelet production. The normal range for MPV is approximately 9 – 12 femtoliters (fL); platelets newly released from the bone marrow are generally larger and, as they age, become smaller. However, interference from similarly sized particles – such as schistocytes or microcytic RBCs – can make the MPV result unreliable. Additionally, the MPV can show greater imprecision or be unmeasurable (suppressed by the analyzer) in samples with low platelet counts.5
Immature Platelet Fraction (IPF)
The Immature Platelet Fraction (IPF%) and Immature Platelet Fraction Count (IPF#) reflect the percentage and absolute number of immature platelets in a patient’s peripheral blood. These immature platelets, newly released from the bone marrow, contain increased amounts of nucleic acid that allow them to be differentiated from mature platelets using fluorescent flow cytometry. Select Sysmex XN-Series™ Automated Hematology Analyzers are capable of reporting the IPF% and IPF# results as a direct cellular measurement of thrombopoiesis, which can be used with other available clinical information to help physicians determine the pathophysiological mechanism of thrombocytopenia.
Clinicians have previously used immature platelet information as a measure of thrombopoietic activity in the bone marrow, which can be important in assessing the likelihood of bleeding. IPF# has been used in clinical trials to assess the treatment effect of thrombopoietin receptor agonists, such as eltrombopag, and has also been studied in patients with immune thrombocytopenia (ITP).6,7
In studies assessing the effect of platelet transfusion on relative and absolute IPF, the IPF% was found to decrease after transfusion due to the increased circulating platelet count, but the IPF# result was not affected, thus “validating the assay as a reflection of ongoing platelet production by the marrow”.8
IPF in the Clinical Setting
Normal Ranges
In 2017, Sysmex determined reference range intervals according the Clinical and Laboratory Standards Institue (CLSI) recommendations. The study of 129 females and 118 males showed the IPF% normal range to be 1.2 - 8.6% and the IPF# normal range to be 3.6 – 20.0 x 103/µL, with no statistically significant difference between the two genders for either parameter. These findings are supported by an independent study published in 2017 based on 2366 samples; however, that study produced a statistically significant difference between the sexes for the IPF% parameter, but not for the absolute IPF.

IPF in the Differentiation of Increased Platelet Destruction versus Decreased Platelet Production
Briggs et al.10 followed AITP (autoimmune thrombocytopenic purpura) and TTP (thrombotic thrombocytopenic purpura) patients with platelet counts of less than 50,000/µL to determine if there is a difference in the IPF between peripheral thrombocytopenia due to bone marrow failure and increased peripheral destruction. The study showed that IPF% values were elevated in both patient groups due to excessive platelet consumption; the IPF% then decreased as the platelet count recovered. These findings were confirmed by Sakuragi et al. in a study that compared IPF% values in patients with primary immune thrombocytopenic purpura (ITP) and aplastic thrombocytopenic disorders.11
A study by Kickler12 at Johns Hopkins looked at IPF values as differentiators in cases of thrombocytopenia. High IPF% values were found in patients with increased production, particularly if associated with platelet destruction, while normal values were seen in decreased platelet production.

IPF in Hepatitis C/Liver Disease
An additional example of the clinical utility of IPF% is the evaluation of thrombocytopenia mechanisms in chronic hepatitis C patients as described by Zucker et al.13 The authors concluded that the IPF% was elevated in thrombocytopenic patients with and withoutsplenomegaly, supporting the idea that peripheral destruction and sequestration are the major causes of the thrombocytopenia in Hepatitis C and liver disease in general.
IPF in Bone Marrow Recovery
Several groups1,4,8,14 have studied the clinical utility of the IPF in varying patient populations: following hematopoietic progenitor cell (HPC) transplantation; myeloablative chemotherapy for hematologic malignancy; disseminated intravascular coagulation (DIC); non-myeloablative therapy in cancer and aplastic anemia; and paroxysmal nocturnal hemoglobinuria (PNH).
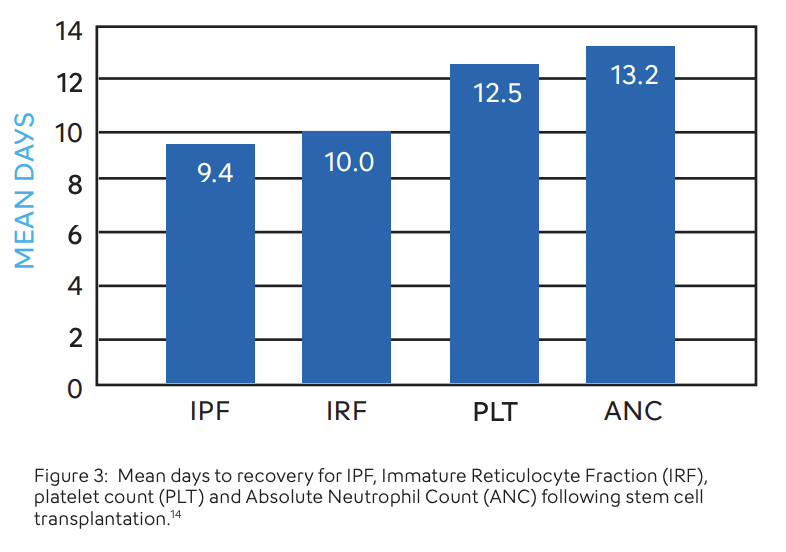
Although it is customary to follow neutrophil recovery after hematologic transplantation procedures, IPF may be another reliable indicator of hematopoietic recovery. Zucker14 and colleagues followed IPF% in 50 patients undergoing peripheral hematopoietic cell transplants and found that IPF recovered, on average, 3.1 days earlier than platelet count alone and 3.8 days earlier than absolute neutrophil counts (ANC). Takami et al.15 also reported the use of IPF as a predictor of platelet engraftment following allogenicstem cell transplantation, findingthat IPF preceded engraftment.Other uses for IPF have beendescribed. Briggs3 et al. havesuggested that the IPF parametermay be able to alleviate the needfor bone marrow examinations aswell as to determine if prophylactic platelet transfusions are necessary for hematopoietic progenitor cell transplant patients.
IPF in Acute Myeloid Leukemia and Myelodysplasia (AML/MDS) Versus Immune Thrombocytopenia (ITP)
It has been difficult to measure platelet function in the presence of severe thrombocytopenia, which is a finding in both AML/MDS and ITP patients. A study conducted by Psaila et al.16 concluded that the difference in bleeding tendencies between these two groups of patients was explained by the quality of the platelets produced. Samples from ITP patients showed younger, larger platelets with increased IPF values versus those from patients with AML/MDS who had lower IPF values and smaller platelets.
IPF in the Assessment of Thrombopoietin Agonists
Another key role of IPF is in determining the efficacy of various treatment protocols for ITP, such as thrombopoietin receptor agonists (TPO-A). A study by Barsam et al.7 showed that patients receiving TPO-A have a higher IPF.
What may be possible with IPF?
- A comprehensive platelet evaluation beginning with a fluorescent platelet count and simultaneous measurement of the IPF to evaluate the maturity of circulating platelets as an indicator of rate of PLT production (thrombopoiesis), i.e., using IPF to assist the physician in defining the best clinical pathway based on destruction/consumption vs. production issues.
- Use of IPF to assess bone marrow recovery and rate of thrombopoiesis.
- Evaluating TPO medication’s effects on thrombopoiesis.
- Evaluating the use of the IPF% parameter as a reflex test in the presence of thrombocytopenia for reporting to hematologists/oncologists.

Conclusion
The Immature Platelet Fraction is a well-studied parameter that offers significant cellular information useful for many patient populations. IPF can function as a routine value reported with every platelet count in certain patient populations or as a reflex test based on your laboratory’s platelet count cut-off. It provides guidance to the physician on the etiology of various thrombocytopenic states, and may help anticipate bone marrow and platelet recovery. Regardless of the application the practitioner chooses, the use of the Immature Platelet Fraction and Count may assist in the delivery of high quality, cost effective patient care.
Keep reading: Download the White Paper