Hemostasis - Prothrombin Time
Download PDF
The Prothrombin Time (PT) test
The PT is a baseline screening test for patients with suspected bleeding abnormalities and continues to be extensively used for monitoring oral anticoagulant therapy (warfarin and other coumadin drugs).
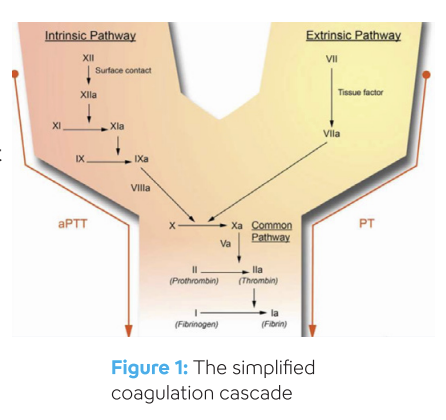
The PT test is not useful for investigating possible causes of clotting in a patient. However, the PT test is useful to assess for defects in the ‘extrinsic’ and ‘common’ pathways of the coagulation cascade (Figure 1). Clotting factors are responsible for ‘normal’ blood clot formation and prevention of bleeding.
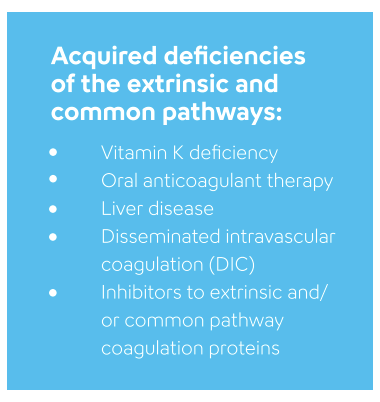
A prolonged (elevated) PT result could be due to reduced or absent activity of one or more of the clotting factors VII, X, V, II and fibrinogen. The reduced activity of these clotting factors could be due to a quantitative deficiency, vitamin K deficiency or an inhibitor directed against the clotting factor.
The PT test was first described by Armand J. Quick in 1935 and was originally developed to measure Factor II (also known as prothrombin). In present day laboratory practice, the sensitivity of the PT test makes it a useful and rapid screening test for deficiencies of the extrinsic and common pathways, whether congenital or acquired.
ISI and INR
Thromboplastin reagent is required for PT testing and generally consists of tissue factor (coagulation factor III), phospholipids and calcium chloride. It is important to understand that different thromboplastin reagents exist for the measurement of the PT test and, therefore, may yield slightly different results. Because of these different sensitivities, it is always important to relate clotting times back to the expected normal range of the reagent being used.
In the early 1980’s, the World Health Organization (WHO) introduced the concept of the International Normalized Ratio (INR) in order to standardize reporting of PT results for patients on warfarin (or equivalent coumadin derivatives). To compensate for the different reagent sensitivities previously mentioned, reagents are assigned an “international sensitivity index” or ISI value. The global standardization of all thromboplastin reagents for oral anticoagulant therapy monitoring requires every lot of PT reagent to be assigned an ISI value. This ISI value is assigned against an International Standard (IS). ISI assignment must be performed for each reagent lot and must also be specific for the technique and measurement principle being used with the reagent. The ideal reagent will have an ISI value of 1.0.
The calculation of the INR is shown here, where MNPT represents the mean normal PT (determined by the laboratory using the thromboplastin reagent in question and the instrument(s) used in the lab for testing patient samples):
INR = (Patient PT / MNPT)ISI
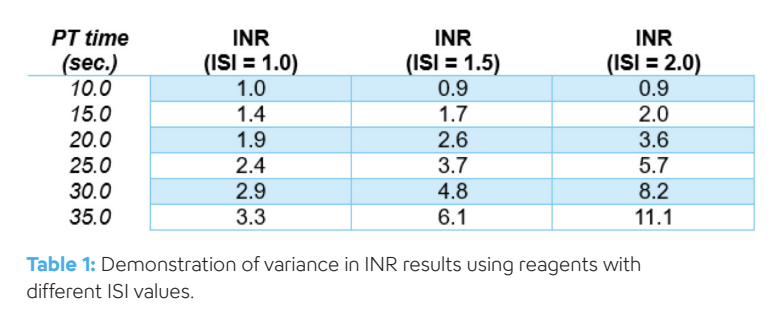
An ISI value close to 1.0 indicates that the PT reagent has good sensitivity to changes in anticoagulant dosing, and therefore it is advisable to use a reagent with an ISI value as close to 1.0, as possible. PT reagents with an ISI value that is close to 1.0 provides better discrimination between normal and abnormal samples in terms of raw PT times (in seconds) as illustrated in Table 1 (pdf).
PT reagents supplied by Sysmex
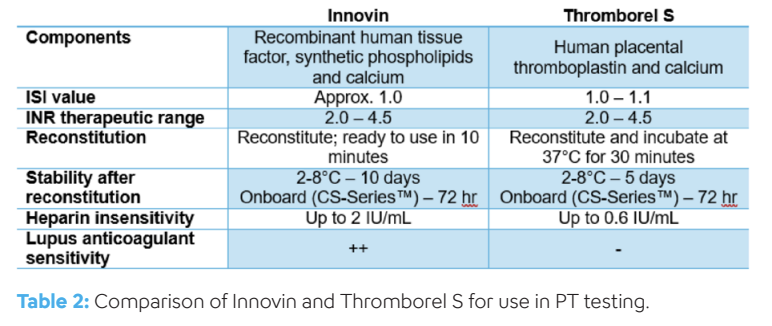
Sysmex currently offers two PT reagents in North America: Dade® Innovin® Reagent (Innovin) and Thromborel® S.
Innovin – Innovin is the most widely used recombinant thromboplastin PT reagent used in the world. Providing consistency and, with an ISI value of approximately 1.0, Innovin demonstrates excellent correlation with the World Health Organization standard. The sensitivity and ease of reconstitution of Innovin, make it the PT reagent of choice for Sysmex customers.
Thromborel S - Thromborel S is prepared from human placental tissue and combined with calcium chloride and stabilizers. Thromborel S has an ISI value of 1.0-1.1 and may be useful for rare patients with a lupus anticoagulant that are on warfarin therapy.
Sigue leyendo Download PDF

