Hemostasis - Laboratory Testing of Hemophilia
Download PDF
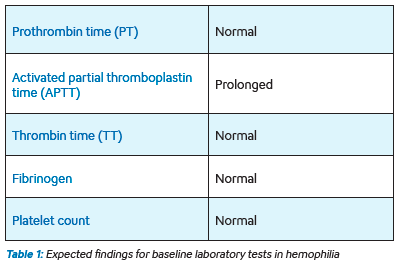
Hemophilia is a bleeding disorder caused by the deficiency of either coagulation factor VIII (FVIII) or factor IX (FIX), called hemophilia A and B respectively. Prolongation of the baseline coagulation screening tests would identify a patient with a clotting factor deficiency. Specific clotting factor assays are needed to identify the specific factor that is deficient. The expected coagulation test result findings in a patient with hemophilia are shown in Table 1 (pdf).
Laboratory testing for hemophilia
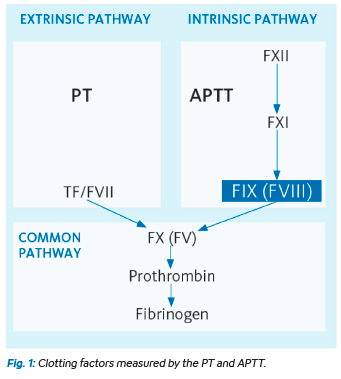
When the APTT is prolonged, correction studies should be performed by mixing the patient’s plasma with normal pooled plasma in a ratio of 1:1. This mixing study is used to determine whether the prolongation of the APTT is due to a factor deficiency – which would correct the APTT – or due to an inhibitor such as heparin – which would not correct the APTT. Figure 1 (pdf) shows the coagulation pathway and the roles played by FVIII and FIX. A deficiency of either of these clotting factors will prolong the clotting time of the APTT to above the normal range.
Individual factor assays must be performed to confirm a diagnosis of hemophilia. Because hemophilia A is far more common than hemophilia B, it is typical to first perform a FVIII assay, followed by a FIX assay if the FVIII level is normal. The test principle and method are essentially the same for both factors, but this section will describe testing for FVIII only.
a)Test principle of the FVIII assay
The activated partial thromboplastin time (APTT) assesses the collective function of coagulation factors that make up the intrinsic pathway and common coagulation pathway (FXII, FXI, FIX, FVIII, FX, FV, FII, fibrinogen). For the APTT to be within the normal range, all the participating factors need to be present in normal or near normal quantities. As all factors are essential for the ultimate generation of a fibrin clot, a deficiency of any one clotting factor will result in a prolonged APTT. The clotting time of the APTT will be prolonged in direct proportion to the extent of the deficiency—i.e., the lower the level of factor, the longer the clotting time. Therefore, if the only variable altering the APTT of a patient sample is the level of a specific coagulation factor, then the value of the APTT can be used to calculate the concentration of the missing factor.
In the FVIII assay, the patient sample with an unknown FVIII level is mixed with a reference plasma which contains normal quantities of all clotting factors except factor VIII—this plasma is referred to as FVIII deficient plasma. By performing this mix, all clotting factor levels are normalized except for FVIII which is the unknown quantity under investigation. Any prolongation of the APTT can therefore be solely attributed to the concentration of FVIII in the patient sample.
b) Reagents and controls required for the FVIII assay
- APTT reagents – the same reagents that are used for baseline APTT testing are required for the intrinsic pathway clotting factor, namely the APTT reagent (Actin FS™) and calcium chloride.
- Reference plasma – this reference plasma (Standard Human Plasma™), which contains a known amount of FVIII, is used to generate a standard curve (calibration curve) against which the clotting time of the patient sample is compared and converted into an absolute value (%).
- Factor VIII deficient plasma – this plasma contains normal amounts of all coagulation factors but is completely deficient in FVIII.
- Normal and abnormal controls – Control Plasma N™ and Control Plasma P™
c) Automated FVIII analysis on Sysmex analyzers
Individual clotting factor assays can be performed on select Sysmex coagulation analyzers. The analyzer needs to be calibrated using Standard Human Plasma whenever the lot number of reagents changes. Please refer to the instructions for use or consult your local Sysmex representative.
d) Results interpretation
The FVIII results are reported as a percentage value. The normal reference range can be quite wide (~50 – 150%) but this is not relevant for the diagnosis of hemophilia. A diagnosis of hemophilia requires there to be an isolated FVIII level below 30% in a male patient. The level of factor will determine the clinical severity and, consequently, the approach to treatment.
What is the role of the laboratory in hemophilia care? Not only are factor assays essential to confirm the diagnosis of hemophilia, but testing is also an essential component of on- going hemophilia care. Hemophiliacs bleed because they have a partial or complete absence of a single clotting factor; namely FVIII or FIX; therefore, the main treatment for bleeding episodes is to replace the missing clotting factor. In order for hemostasis to be effectively restored, clotting factor levels must reach a certain minimum level. It is therefore vital that factor levels are checked at specific time intervals after the factor concentrate has been administered. Algorithms exist which assist in determining how many units of FVIII for FIX need to be infused based on the patient’s factor level and the body weight. This is used to determine the starting dose of factor concentrate, but the response to treatment must be confirmed by repeating the factor assay post-infusion. If the recovery of the factor level is sub-optimal, then a top up dose must be given, especially if there are still clinical signs of bleeding. If patients do not respond as expected or require ever increasing doses to control bleeding in comparison to previously, the possibility that inhibitors have developed must be explored.
What are inhibitors?
One of the most serious complications that arise from hemophilia treatment is the development of antibodies, or inhibitors, against the infused factor concentrate. This tends to occur only in patients with severe hemophilia where there is less than 1% or a complete absence of factor. Because the patient has virtually no endogenous FVIII (or FIX), any infused exogenous factor is seen by the body as a foreign substance against which antibodies are produced. These antibodies are referred to as inhibitors as they bind to the infused factor and prevent it from participating in the coagulation cascade. This means that larger quantities of infused factor are required to sustain coagulation. This occurs in approximately 5 to 10% of patients with severe hemophilia A and 2 to 4% in patients with severe hemophilia B.
Sysmex Testing Solutions
Hemophilia patients are at risk of bleeding (internally and externally) due to reduced/absent functional factor VIII or IX in their blood. While proper diagnosis of hemophilia is crucial, management of hemophilia is equally important, since this is a life-long disorder.
The testing for diagnosis of hemophilia A and treatment monitoring of hemophilia A generally differ. Laboratories utilizing Sysmex CS-Series and CN-Series analyzers* have access to industry-leading reagents and advanced technology to provide the accurate results required for the management of these patients.
One-stage Factor VIII assay (primarily used in diagnostic testing)
- Requires the following reagent products (sold separately):
- Factor VIII deficient plasma
- Actin FS or Actin FSL – APTT reagent
- Calcium chloride
- Owren’s Veronal Buffer (OVB) – for automatic sample dilutions performed by the analyzer
- Standard Human Plasma (SHP) – for calibration curve generation
- Control N - Normal level QC
- Control P - Abnormal level QC
Factor VIII Chromogenic assay (primarily used in management testing)
- Requires the following reagent products (sold separately):
- Factor VIII Chromogenic kit
- OVB – for automatic sample dilutions performed by the analyzer
- SHP – for calibration curve generation
- Control N - Normal level QC
- Control P - Abnormal level QC
*Analyzers not available in all markets.
Keep reading: Download PDF


