Hematology - White Paper Erythrocyte Sedimentation Rate
Download PDF
Technology, correlation and reference range considerations
Introduction
The erythrocyte sedimentation rate (ESR) is widely used as a screening test that indirectly and non-specifically
measures the presence of inflammation. Elevated ESR results may be seen in a variety of conditions including
infections, malignancies, renal disease, inflammatory states and autoimmune diseases.
Traditionally, the ESR has been measured using EDTA anticoagulated whole blood which is diluted and placed into a specialized glass tube and allowed to sediment over a one-hour period. After the one-hour sedimentation period, the height of the red blood cell (RBC) column is measured to determine the distance the RBCs have settled. While simple to perform, manual ESR methods are time consuming, labor intensive and increase the potential for operator exposure to biohazardous materials. Additionally, manual ESR methods are impacted by numerous other factors including: environment (vibration, temperature fluctuation and drafts in the test area), sample specific conditions (anemia and abnormal RBC morphology) and operator technique (setting up the test and reading the result).1
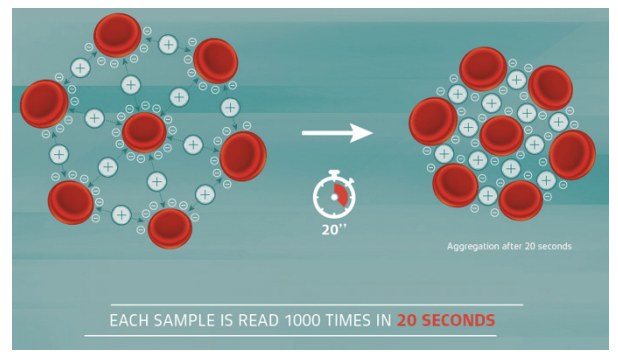
Normal RBCs have a net negative charge which causes them to repel each other. An increase in proteins like fibrinogen, alpha and beta globulins and immunoglobulins reduces the net negative charge of the RBCs. This promotes formation of rouleaux and agglutination which causes the RBCs to sediment more quickly and increases the ESR. Erythrocyte sedimentation occurs in three stages: rouleaux formation in which RBCs aggregate for the first 10 minutes; sedimentation, which occurs over the following 40 minutes; and RBC packing, which occurs in the last 10 minutes. Despite the test name and reporting units of millimeters/hour, the ESR is not timing the rate of sedimentation. Rather, it is a measurement of the amount of sedimentation as determined by the height of the RBC column at one hour. Various ESR methods may not consider all phases of sedimentation and can be susceptible to different interferences and proteins generated in diverse disease states.
The Alifax® Erythrocyte Sedimentation Rate Analyzer Series uses capillary photometry technology which eliminates the disadvantages of the manual ESR method; by providing ESR results in 20 seconds, laboratory efficiency and turn-around-times are improved. Capillary photometry technology is listed in the Clinical and Laboratory Standards Institute guideline for ESR testing (H02-A5) as an alternative to traditional ESR methods.2 Proficiency testing samples for the Alifax systems are available from proficiency testing providers such as the College of American Pathologists.
Specimen requirements
Specimens must be collected in either K2 or K3 EDTA
anticoagulant. Optimal time to analyze a specimen
stored at room temperature is within 4 hours of
collection. Refrigerated specimens are acceptable for
testing for up to 24 hours after collection. The sample
must be allowed to come to room temperature for
approximately 15 minutes before testing. Refer to the
analyzer instructions for use for more information on
specimen collection and handling.
Alifax systems do not require the use of special collection tubes for determination of ESR results. One EDTA tube can be used for all routine hematology testing, decreasing collection tube costs and increasing pre-analytic efficiencies. Unlike systems which read the ESR result through the tube wall, the Alifax systems perform closed tube sample aspiration, eliminating interference from excessive tube labels.
Correlations
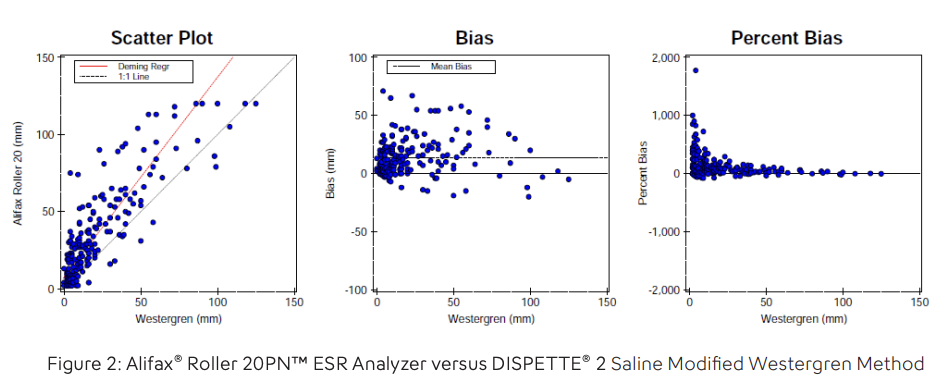
A correlation study was performed by Sysmex using
201 fresh, whole blood samples collected in K2-EDTA
from an acute care hospital comparing the Alifax®
Roller 20PN™ ESR Analyzer and the DISPETTE® 2
Saline Modified Westergren method. The samples
were processed first on the Alifax Roller 20PN with
no pre-mixing before analysis. The internal analysis
mode with analyzer sample
mixing was used for all samples
tested on the Alifax system. After
processing on the Alifax system,
the samples were tested using
the DISPETTE method according
to manufacturer’s instructions.3
All test setup and resulting
was completed by the same
laboratory scientist to eliminate
operator-to-operator variability
associated with the manual ESR.
Results on the Alifax Roller 20PN ranged from 2 to 120 mm. Using regular linear regression to analyze the data, the slope was 1.064 (95% Confidence Interval [CI] 0.973 to 1.156), the intercept was 12.5 (95% CI 9.5 to 15.5) and the correlation coefficient (R) was 0.8526.
The ESR is measuring the phenomenon of RBC sedimentation which is impacted by the presence of various plasma proteins and sample specific factors. It is not measuring an actual analyte such as hemoglobin or cholesterol. Tests for analytes like hemoglobin and cholesterol are highly standardized between manufacturers and calibrated with calibrators traceable to a reference method. There is not an internationally recognized calibration standard for the ESR. It is important to note that, because of how the ESR is measuring the phenomenon of RBC sedimentation rather than an analyte (such as hemoglobin or cholesterol in an end-point photometric reaction) there can be more imprecision with ESR results. Due to these factors, comparison studies between different ESR methods may not show the high degree of correlation that one would expect with a highly standardized analyte. The phenomenon of erythrocyte sedimentation is impacted by the effect of all the various plasma proteins as well as other sample related factors. Because of this, ESR results may not correlate to C-reactive protein (CRP) and fibrinogen results.
Reference ranges
Due to the many factors that influence the ESR,
laboratories have historically used reference ranges
obtained from literature when reporting ESR results.
Intensive screening to identify truly ‘normal’ subjects
would be necessary when performing an ESR
reference range study.
This would involve excluding subjects from the study if they had any of following conditions:
- History of autoimmune, inflammatory disorders or diabetes
- Taking any medicines or supplements
- Tobacco use
- Ethanol use
- Pregnancy
- Menstruating
- Recent injury or surgery
- Elevated biochemical markers of inflammation like CRP or fibrinogen
Since ESR results are age and gender dependent, sufficient ‘normal’ subjects for males and females in different age ranges would also be required. Such a reference range study to identify ‘normal’ subjects is not possible or practical. This is similar to other analytes like tumor markers or therapeutic drugs which require extensive clinical or other evaluation to determine a reference range.
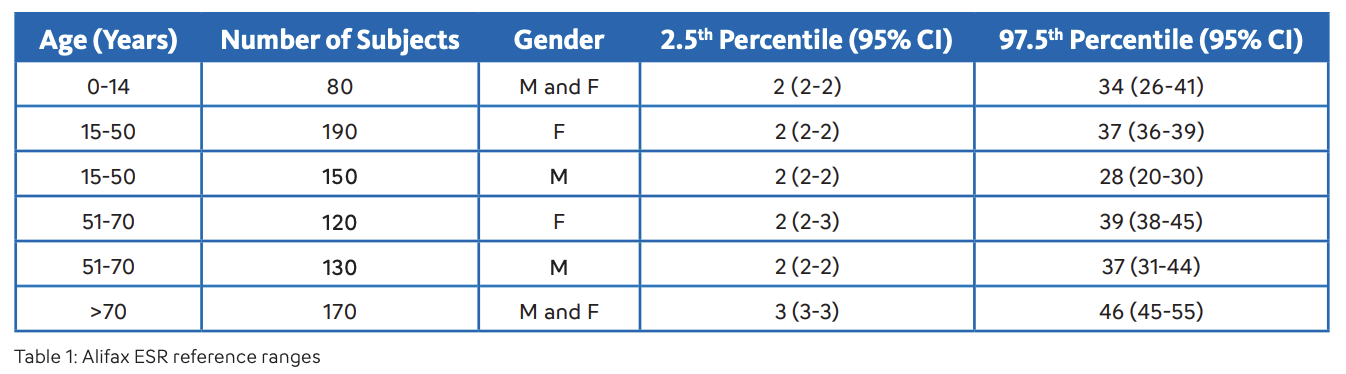
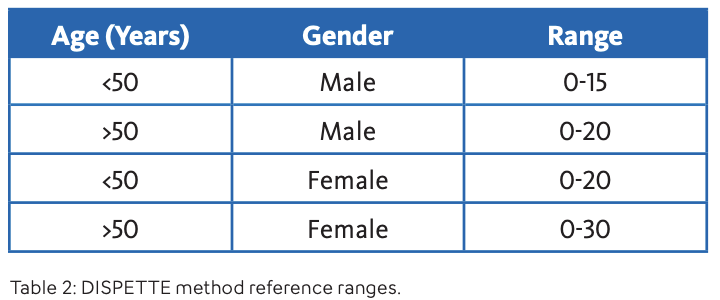
An extensive reference range study, excluding subjects meeting the above criteria, was performed by Piva et al.4 to determine the reference ranges for the Alifax ESR method (Table 1). A concordance study was performed by Sysmex using 100 fresh K2-EDTA whole blood samples. Samples were residual samples from male and female patients ranging in age from 18 to 94. Samples were tested using the Alifax Roller 20PN and the DISPETTE 2 Saline Modified Westergren method. Considering the age and gender of the patient, results were classified as normal or abnormal using the reference ranges shown in Table 1 for the Alifax method. For the DISPETTE method, reference ranges from Clinical hematology: Principles, procedures, correlations5 (Lotspeich-Steininger, et al) were used and are shown in Table 2.
Of the 100 samples, 84 had the same interpretation (normal or abnormal) considering the reference ranges for each method. Of the 16 samples with discordant interpretations, 9 samples had results that were borderline and near the upper limit of the reference range for one or both methods. Some discordant result interpretations are expected when comparing ESR results from differing methodologies. This may possibly be due to the presence of plasma proteins associated with certain disease states or other sample specific factors.6
To monitor disease progression in certain clinical states (i.e., rheumatic disease or multiple myeloma), some clinicians monitor ESR results over time. When changing ESR methodologies, laboratories should consider notifying ordering clinicians of the method change. Another option is to report all ESR results with a message about the method change for a time after going live with the new methodology. This will help raise awareness with clinicians that a change in the result is likely due to the method change rather than a change in the patient condition.
Summary
Automated systems such as the Alifax family of ESR analyzers provide results more quickly and efficiently
than manual ESR methods. They also eliminate the issues associated with the manual ESR method including
influences from environmental factors and operator-to-operator technique variability.
Different ESR methods can have varying susceptibilities to interferences and proteins generated in different disease states. Method specific reference ranges should be adopted when implementing new ESR methodologies.
Bibliography
1. Jacobs, David S., Dwight K.
Oxley, and Wayne R. DeMott.
Jacobs & DeMott, Laboratory
Test Handbook, Hudson
(Cleveland), OH: Lexi-Comp,
2001.
2. “H02-A5, Procedures for the Erythrocyte Sedimentation Rate Test, 5th Edition”, Clinical and Laboratory Standards Institute, Wayne, PA, May 2011
3. DISPETTE® 2 Saline Package Insert (FH1600), March 2016. Sedimentation Rate): Variations with Sex and Age and Reference Limits. Clinical Chemistry and Laboratory Medicine, 39(5), pp. 451-454. Retrieved 4 Dec. 2018, from doi:10.1515/ CCLM.2001.071.
4. Piva, E., Sanzari, M., Servidio, G., et al. (2005). Length of Sedimentation Reaction in Undiluted Blood (Erythrocyte Sedimentation Rate): Variations with Sex and Age and Reference Limits. Clinical Chemistry and Laboratory Medicine, 39(5), pp. 451-454. Retrieved 4 Dec. 2018, from doi:10.1515/ CCLM.2001.071.
5. Lotspeich-Steininger, C. A., Stiene-Martin, E. A., & Koepke, J. A. (1992). Clinical hematology: Principles, procedures, correlations. Philadelphia: Lippincott.
6. Kim M, Ju Y-S, Lee EJ, et al. Erythrocyte sedimentation rate measured using microhemagglutination is not elevated in monoclonal gammopathy compared with other diseases. Int J Lab Hem. 2018;40:540–548. https://doi. org/10.1111/ijlh.12859. 4. Piva, E., Sanzari, M., Servidio, G., et al. (2005). Length of Sedimentation Reaction in Undiluted Blood (Erythrocyte
Keep reading: Download PDF